 Apollo Hospital
Apollo Hospital Fortis Hospital
Fortis Hospital Artemis Hospital
Artemis Hospital
 Medanta Hospital
Medanta Hospital



 Jaslok Hospital
Jaslok Hospital Lilavati Hospital
Lilavati Hospital

 Global Hospitals
Global Hospitals Jupiter Hospital
Jupiter Hospital
Colorectal Surgery in India
 Colorectal surgery repairs damage to the colon, rectum, and anus through a variety of procedures that may have little or great long-term consequence to the patient. It may also involve surgery to the pelvic floor to repair hernias.
Colorectal surgery repairs damage to the colon, rectum, and anus through a variety of procedures that may have little or great long-term consequence to the patient. It may also involve surgery to the pelvic floor to repair hernias.
Gastro-intestinal surgery in general and colonic surgery in particular is considered as very demanding and requires - high degree of operative skill. Major breakthrough was achieved when end to end anastomosis (E.E.A.®.) stapler was introduced in the year 1979 by United States surgical corporation (U.S.S.C.®). In Indian set up the 1st use of staplers was in the year 1981 and gradually it gained popularity.
Colon Cancer Surgery in India
Vital Information
Phone : +91-9371136499/ Whatsapp : Chat
Chat
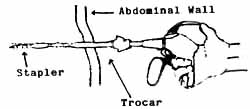
All these years surgeons have been inflicting injuries to abdominal wall to get access to internal organs inorder to achieve cure. Minimal invasive surgery (M.I.S.) in the discovery of the last decade is an attempt to minimise these injuries for patients benefit. A breakthrough of last millennium. Dr. Kurt Semm a gynaecologist from Germany performed the first laparoscopic appendicectomy in the year 1981. Another German surgeon Dr. Eric Muhe in the year 1985 performed the world's first laparoscopic cholecystectomy. Big abdominal incision for majority of intraabdominal diseases is a thing of the past.
Laparoscopic colonic surgery is being accepted by many centres as primary line of treatment for carcinoma colon. It is no more considered an experimental work. Centres specialised in this field have conducted double blind randomised trial (DBRT) in large number of cases and have shown that the basic principles of oncosurgery are not compromised and long term follow-up results are comparable to conventional surgery. In India because of limited work load of colonic cancer, it has not made the progress unlike laparoscopic cholecystectomy. There are no large published series. We have carried out 32 colonic surgeries, out of which only six are for malignancy, the rest being inflammatory colonic diseases.
It makes great sense to offer the benefits of M.I.S. to our patient in terms of :
- Less post operative pain and analgesics.
- Shorter hospital stay.
- Less wound related and post-op pulmonary complication.
- Early return to work or family.
- Better cosmesis.
Port site implantation was a concern in early period but it has been shown now that it can be prevented by
- Proper protection of port site while delivering the specimen. (Endobags ® and pouches).
- Avoid squeezing of the specimen by taking a liberal incision.
- Thorough wash to the wound, 5FU solution irrigation of all ports.
- Slow release of pneumo-peritoneum.
- Lap-lift technique etc.
It has been reported that in conventional surgery also scar metastasis rate is about 2.5 per cent and by above mentioned guidelines the reported large series quite a port site metastasis to the tune of 1 to 2.5% only. Cost can be brought down by either doing a hand sewn anastomosis through the specimen delivery site or use of conventional stapler for extra - corporeal stapled anastomosis. Minimal use of disposable trocars and instruments can further cut down the cost. Use of ultrasonic energy source in form of harmonic shears (Ethicon ® and U.S.S.C.®) has added to the cost of lap surgery.
Harmonic disposable hand pieces are reused by us multiple times to cut down the cost. Tremendous amount of time and blood loss is saved particularly in obese patient by use of ultrasonic generator. We have observed that the same can be achieved to a great extent by use of bipolar diathermy endo-scissors, dissectors and hooks etc. The sealing capacity for vessels is comparable and no lateral thermal damage takes place when bipolar electric energy source is used. Haemostasis in our initial cases was carried out by use of bipolar diathermy and of late we carry out these procedure with much ease by Harmonic scalpel ultracision (L.C.S. of Ethicon). In fact we are the first to acquire this in Mumbai's private setup.
The two burning issues are port site metastasis in malignancies and cost factor due to use of endostaplers. As mentioned earlier for benign condition like rectal prolapse, adenomas, rectal polyposis and inflammatory condition like tuberculosis, ulcerative colitis, simple diverticulitis, laparoscopic surgery offers a patient friendly technique. Crohn's though not very common in our country, but laparoscopy can be offered for diagnosis, lymph node sampling and curative resection. Ileo-caecal tuberculosis is commonly seen in our country and its a good option to offer the benefits of M.I.S. to these patients whenever surgery is indicated. Incidental colonic resection is unlikely to help the laparoscopic surgeon team in mastering the techniques. Reduction of O.T. time due to better co-ordination and cost benefit to patients can only be offered by repetitive performances. A dedicated team effort will surely bring this speciality under the umbrella of M.I.S. as has happened in western world. Details of various procedures is beyond the scope of this article, but I will give a broad overview of various procedures.
Diagnostic laparoscopy
- This is offered to stage a malignant condition, take tissue for biopsy and have relook (second look) operation by laparoscopy.
- To obtain specimen and lymph nodes in inflammatory large bowel diseases.
Laparoscopic colostomy
Laparoscopy is mainly used to achieve faecal diversion in unresectable malignant growth, severe perianal infections, trauma faecal incontinence and complex fistula in ano. If indicated even a loop iliostomy can be offered to patient.
Laparoscopic colonic resection
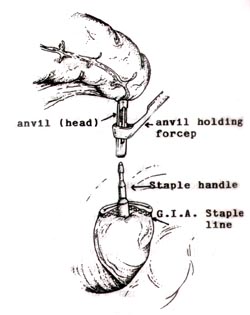
Rt and Lt hemicolectomy, total colonic resection, abdomino-perineal resection (APR), anterior resection (AR), lap assisted resection[3] are various procedures that can be offered to patients. Out of these the most difficult technique is a transverse colonic resection in an obese patient. Large malignant and inflammatory masses also are relative contraindication for surgery. Obstructed lesions are absolute contraindication for Lap surgery. To resect the bowel Endo-staplers can be used. Now we have even smaller stapler in the form to endo G.I.A. 30 (Fig. 1). Smaller length is easy to handle and manoeuvre. If larger lumen needs to be divided, it's better to fire smaller endo G.I.A. 30 twice. Variable staple height of 2 mm, 2.5 mm, 3 mm colour coded cartridges are used according to bowel thickness (Fig. 2). Vascular pedicles can also be divided by using 2 mm height stapler. We prefer to tie the vessels individually at the root of mesocolon is gives better nodal clearance and cuts down the cost. For anterior and low anterior resection EEA® cured staple became very handy (Fig. 3). Proper selection of size is very essential to form a proper anastomosis. Three sizes are available 25 mm, (28-29 mm), (32-33 mm) giving an inner stoma of 15 mm, 19 mm and 22 mm.
Showing staple height, staple line of 3 rows on each side with line of cutting and closure of staple in letter B format

Complication of lap colonic surgery are the same as conventional surgery namely:
- Bleeding.
- Anastomotic leak.
- Infection.
It has been observed that bowel function returns much earlier in lap surgery. Thus feeding is started much earlier and hospital stay is shorter. The reason for early return of peristaltic activity is lack of handling and non-exposure to outside atmospheric air. Flatus, faeces and feeds (three F's) of colonic surgery are much faster in M.I.S.
Dissection of specimen removed after laparoscopy have been compared with conventional surgery specimen in terms of
- Number of lymph node harvested.
- Resected margin clearance.
- Length of specimen.
It has been seen that the basic principles of oncosurgery are not compromised. The procedure done is same as open surgery. The five year survival rate are comparable.
It has been reported that laparoscopic surgery offers less immuno - supression post operatively as compared to conventional surgery. Surgeon should not hesitate to convert in difficult situation, keeping in mind the patient safety. Average conversion rate is 10 to 12% in malignancy and 18 to 20% in inflammatory colonic condition.[5] Procedures are not to be compared but comparison of surgeons philosophy and sound judgement gives different conversion rates. Ileal pouch after total procto-colectomy can easily be fashioned with G.I.A. 90 mm. Harmonic scalpel if available reduces the blood loss and O.T. time.
Prolapse rectum requiring surgery is another condition wherein the benefits of laparoscopic surgery can be offered to the patient. Various types of procedures are carried out.Surgeon has to be proficient in the art of laparoscopic knotting and suturing. In absence of that various fixing decision like stapler and Tacker ® can be used to fix the mesh in place. We have one of the largest series of laparoscopic rectopexy. We prefer Notora's modification of Ripstein technique. So far 16 such procedures are carried out with good results.
Rectosigmoidectomy and anterior resection are other procedures carried out. Proper selection of patients and right procedure offered will give long lasting results.
Colorectal Surgery in India is available in following cities
| Mumbai | Hyderabad | Kerala |
| Delhi | Pune | Goa |
| Bangalore | Nagpur | Jaipur |
| Chennai | Gurgaon | Chandigarh |
Go to the Enquiry Form
Phone Numbers Reach Us
India & International : +91-9860755000 / +91-9371136499
UK : +44-2081332571
Canada & USA : +1-4155992537
Below are the downloadable links that will help you to plan your medical trip to India in a more organized and better way. Attached word and pdf files gives information that will help you to know India more and make your trip to India easy and memorable one.
Click icon to Download Document
| About India |
|
|
Destinations in India |
|
|
|
| Indian Embassy List |
|
|
Medical Tourism FAQ |
|
|
|
| Visa For India |
|
|












