 Apollo Hospital
Apollo Hospital Fortis Hospital
Fortis Hospital Artemis Hospital
Artemis Hospital
 Medanta Hospital
Medanta Hospital



 Jaslok Hospital
Jaslok Hospital Lilavati Hospital
Lilavati Hospital

 Global Hospitals
Global Hospitals Jupiter Hospital
Jupiter Hospital
Gastric Intestinal Resection Surgery India
Intestinal Resection:
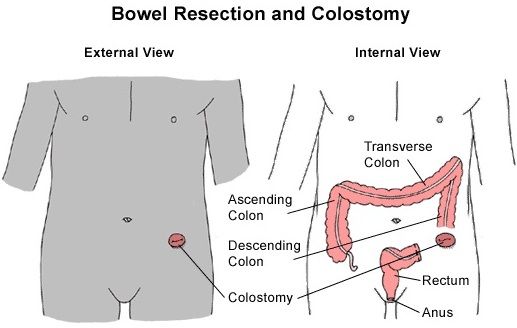
INTESTINAL RESECTION AND ANASTOMOSIS
GENERAL INFORMATION
- End-to-end anastomosis is the gold standard.
- If the luminal diameter post-transection is anticipated to be unequal, use a perpendicular incision across the intestine with the larger luminal diameter and an oblique incision across the area with the smaller diameter.
- Make the oblique incision so the antimesenteric border is shorter than the mesenteric border.
- With equal luminal diameters, use a perpendicular incision.
- Intestinal healing is dependent upon blood supply, mucosal apposition and amount of surgical trauma.
- Approximating sutures will facilitate the most rapid intestinal healing.
- Intestinal suture patterns need to include the tough submucosal layer, so be sure to incorporate it in your sutures. Omental wrap or pexy.
- Do not use catgut or multifilament suture materials when closing intestinal incisions.
MOST COMMON COMPLICATIONS AND DIFFICULTY
- Dehiscence and leakage are the most common severe complication. Use proper technique to avoid this complication.
- Tissue trauma/maceration from rough handling with traumatic forceps during suturing.
- Removal of more than 70% to 80% of the small intestine may result in short bowel syndrome.
Effect of intestinal resection on human small bowel motility
Few data are available on adaptive changes of human small bowel motility after intestinal resection. AIM: To characterise jejunal motility after extensive and limited distal intestinal resection. METHODS: Seven patients with a short bowel syndrome after total ileal and partial jejunal resection (residual jejunal segments between 60 and 100 cm) and six patients with limited distal ileal resection (resected segment between 30 and 70 cm) underwent ambulatory 24 hour jejunal manometry 15 (6-24) months after the operation. Normal values were obtained from 50 healthy subjects. Fasting motility and the motor response to a 600 kcal solid meal were analysed visually and by a computer program. RESULTS: Limited ileal resection did not result in changed jejunal motility. After extensive distal resection, patients had a significantly shorter migrating motor complex (MMC) cycle and a significantly shorter duration of the postprandial motor response compared with controls (p < 0.005). Intestinal resection had no influence on jejunal contraction frequency and amplitude and did not lead to any abnormal motor pattern. CONCLUSION: Extensive distal resection of the small intestine produces distinct abnormalities of fasting and postprandial motility in the intestinal remnant. The shortening of digestive motility and the increased frequency of MMC cycling could contribute to malabsorption and diarrhoea in the short bowel syndrome.
EXPERTS' ADVICE
- Gently reflect mesenteric fat from ends of bowel to identify bowel wall.
- Place stay sutures at the mesenteric and anti-mesenteric borders to begin the closure. This allows proper alignment and the best apposition and suture placement at the mesenteric border.
- Place atraumatic forceps (Doyens, assistant’s fingers, arms of Allis tissue forceps) at least one arcuate vessel away from the anastamosis site to prevent compromise to the blood supply at the anastamosis.
- The mesenteric border is most likely to leak. Begin your closure there and be sure that you incorporate the submucosa in your sutures.
- Consider using a serosal patch if delayed healing is expected.
Gastric Intestinal Resection Surgery in India is available in following cities:
| Mumbai | Hyderabad | Kerala |
| Delhi | Pune | Goa |
| Bangalore | Nagpur | Jaipur |
| Chennai | Gurgaon | Chandigarh |
Go to the Enquiry Form
Phone Numbers Reach Us
India & International : +91-9860755000 / +91-9371136499
UK : +44-2081332571
Canada & USA : +1-4155992537
Below are the downloadable links that will help you to plan your medical trip to India in a more organized and better way. Attached word and pdf files gives information that will help you to know India more and make your trip to India easy and memorable one.
Click icon to Download Document
| About India | Destinations in India | |||||
| Indian Embassy List | Medical Tourism FAQ | |||||
| Visa For India |












